
Getty Images/iStockphoto
How COVID-19 Imperiled Physician Practices, And How to Save Them
Physician practice revenue has been cut in half during the early part of the COVID-19 pandemic. Could telehealth and payment reform save the independent physician?

Some have heard the ringing of the death knell for physician practices for years now. Mergers and acquisitions, industry consolidation, value-based care, and the growing presence of private equity firms in healthcare have all threatened the survival of the practice.
But the COVID-19 pandemic could be the nail in the coffin for even the strongest physician practices.
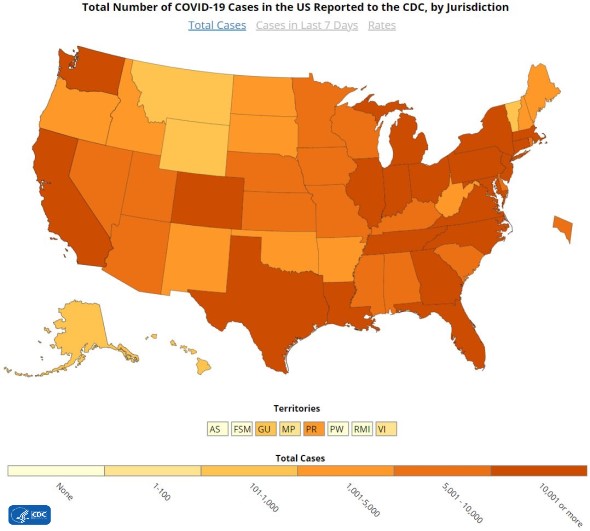
HHS Secretary Alex Azar declared COVID-19 a public health crisis on January 31, 2020. Since then, the number of new cases in the US rose from the single digits to over 1 million confirmed cases, according to data collected by Johns Hopkins University at the time of publication.
The highly contagious novel coronavirus has upended operations for hospitals, which have had to build staff, capacity, supplies, and other necessary capabilities to treat this sudden surge in infected patients. But the outbreak has also had a profound impact on ambulatory care.
A survey conducted April 10 to 13 by the Primary Care Collaborative and The Larry A. Green Center found that half of primary care practices are unsure if they have enough cash to keep their practices open. With that being the case, one in five surveyed primary care practices anticipated closing within four weeks.
“Our sample size was 2,600 practices that week, and an additional 40 percent said that they were unsure,” said the survey’s lead author Rebecca Etz, PhD, co-director of The Larry A. Green Center and associate professor of family medicine and population health at Virginia Commonwealth University.
“That is a dramatic and immediate public health crisis that requires dramatic and immediate attention,” she recently told RevCycleIntelligence.
How COVID-19 is impacting physician practices
Jonathan Lilly, MD, is used to having a full schedule.
A board-certified family practitioner, Lilly is one of seven physicians at Dunbar Medical Associates, PLLC. As an NCQA-certified patient-centered medical home and an accountable care organization (ACO) practice through Aledade, Dunbar Medical Associates is entrenched in the value-based care model, which has filled Lilly’s schedule in the past.
“Our outreach and follow-up to keep people healthy have kept us with busy schedules. Now, we’re doing about 60 to 70 percent of what our usual volume is,” he recently said in an interview.

The COVID-19 pandemic has forced Dunbar Medical Associates and practices like it to cancel or postpone many of the procedures and services that keep patients healthy and subsequently generate revenue.
Patients have stopped seeking care out of fear of exposure and CMS and state governors have advised providers to delay non-emergent, elective medical services to reduce the burden COVID-19 has on the healthcare system.
These factors have led to an average 60 percent decline in patient volumes since the start of the public health emergency, the Medical Group Management Association (MGMA) recently reported. As a result, physician practice revenue has been cut in half.
“We're doing something we've never had to do before, which is helping patients to stay away, finding reasons for people not to visit,” says Daniel M. Duncanson, MD, CPE, CEO at SIMEDHealth in Florida. And the way the fee-for-service system is structured is creating revenue problems during the pandemic.
“It’s the loss of healthier people getting procedures that are not necessarily elective but aren't life-threatening. It's the loss of the imaging and the ancillaries that are associated with those services,” he explained.
“As a physician, I can do about 80 to 90 percent of what I need to do by telehealth, but that extra 10 to 20 percent is still an important percent and that's being given up on healthcare right now.”

Without those revenue-generating services, SIMEDHealth has had to cut down hours and consequently compensation for some of its 100-plus physicians. Some staff have also been furloughed to conserve cash reserves.
Physician practices and medical groups are increasingly having to make these tough decisions. About 21 percent of physicians have been furloughed or had their pay cut during the COVID-19 crisis, revealed a new survey from Merritt Hawkins and the Physicians Foundation.
The COVID-19 pandemic has also spurred more physicians (32 percent) to consider leaving direct patient care roles altogether.
The findings hint at what Etz described as a “public health crisis that is living underneath the pandemic.”
“We fear that many practices will close because of a lack of patient volume or lack of payment to cover costs at just the time when patients need us most,” Etz said. “If primary care goes down, the rest of the US healthcare system goes down with it.”
Telehealth to the rescue
With social distancing and stay-at-home orders in effect, in-person visits have dramatically decreased, and in some cases, completely stopped. But providers are finding new ways to connect with their patients and keep the lights on.
Telehealth implementation has emerged as one of the silver linings from the pandemic, according to Richard Harris, MD, president of LUGPA and a board-certified urologist practicing at UroPartners in Illinois.
“If there is anything that can be said as a positive which has come out of this nightmare, it’s that we have been able to utilize telemedicine which was not available to the masses in the past,” said Harris.
Physician practices have yet to report the wide-scale adoption of telehealth technology that hospitals and health systems have. Only about 15 percent of physician practices were using telehealth for patient care as of last year, and even fewer (11 percent) were using the technology to communicate with other providers, a study from the American Medical Association (AMA) found.
But since the outbreak, physician practices have rapidly acquired and implemented telehealth systems.
“We had not used it at all. Now, we are doing about 70 percent through telehealth,” reported Lilly.
Physicians around the country are similarly ramping up telehealth services during the pandemic and finding that the technology is not the big bad wolf it appeared to be.
“I'm not the savviest IT person in the world and I've been utilizing it. It's very simple to get engaged,” Harris stated.
The technology is filling a glaring gap in ambulatory care that has been more pressing with the outbreak of a highly contagious virus and new social distancing protocols. But the real reason why practices have been able to so quickly implement and scale telehealth rests with regulation.
“None of the insurance companies nor the government reimbursed for it unless you were in a rural setting,” Harris explained. The Coronavirus Aid, Relief and Economic Security (CARES) Act changed that.
Passed in late March, the CARES Act dedicated pages of legislation and billions in emergency funding to healthcare providers, including Medicare reimbursement and payment parity for using telehealth to treat seniors at home. The law paved the way for a flurry of other telehealth flexibilities for Medicare and Medicaid providers, including getting paid for more virtual services furnished by a longer list of clinicians.
This revenue is keeping physician practices afloat during a public health emergency that turned into an international financial crisis.
About a third of physician services are now eligible for telehealth reimbursement under traditional Medicare, with some specialties having 90 percent or more of Medicare payments eligible for reimbursement via telehealth, consulting firm Avalere recently reported.
However, many practices have yet to experience the financial bump from coverage changes.

“Medicare has already made some dramatic shifts in their policies, and they are paying for telehealth and virtual health on parity, at least for the moment. It’s unclear whether those policies will extend past the pandemic. Private insurers are not yet doing so and they need to,” Etz explained.
Etz’s survey has shown that 60 percent of primary care clinicians have consistently reported that the majority of their work is not reimbursed or funded, and a large portion of that work is telehealth.
“Practices are doing what's best for population health to their detriment,” Etz stated.
The pressure is on private payers to step up to the plate. Congress and major healthcare advocacy groups are calling on them and CMS to pay providers the same rates as in-person visits during the pandemic to bolster the healthcare system’s response to COVID-19 and even beyond.
“There will be a unanimous cry from healthcare providers and associations if CMS just turns the light switch off on this for the very real reason of safety,” said Duncanson. “I don't think any of us believe that social distancing is just going to stop, and everything is going to go back the way it was pre-March. This is going to be a phased-in thing and the sickest of the patients are the ones that we need to continue to be able to see to provide care for and get reimbursed for in a virtual modality.”
Telehealth reimbursement and other regulatory flexibilities could also prevent physician practices from such dire straits in the future.
Surviving in a COVID-19 world
March and April were troubling months for healthcare organizations and some communities have yet to hit the peak of COVID-19. Organizations across the board are preparing for rocky second and third quarters, but many industry experts agree that this isn’t just a passing phase.
“I don't know that there is a ‘go back to normal.’ At this point, I think that healthcare in the US has been changed forever,” Etz stated.
Many physician practice leaders are preparing for this new normal. The current administration has already released its plans for reopening the economy, but fully restoring the healthcare system will take awhile and practices could be implementing social distancing protocol for a lot longer.
Practices like SIMEDHealth are already determining how to continue protecting patients and staff through screenings and designated spaces for sick patients even though there could be a tsunami of patient care when social distancing recommendations are lifted.
This could mean reduced revenues well through the summer, Harris predicted. With the typical two-month lag with claims reimbursement, Harris would not be surprised if revenues were less than 50 percent what practices are used to by the fall and even the winter.
But the COVID-19 pandemic will serve as a catalyst for change that can help practices weather the next storm. For one, it could mean a more permanent place for telehealth in ambulatory care.
Supporting telehealth through payment could prepare primary care for future viral outbreaks.
“If somebody has the flu or if COVID-19 comes back, you'll be able to see them remotely, take care of them, and get them tested while limiting exposure and continuing the other part of the business,” said Lilly.
Paying practices to implement and use telehealth could also prove useful for non-coronavirus work. While on call during the nights and weekends, telemedicine would add value in having patients and physicians have face-to-face contact and enhance communication further enhancing the patient-physician relationship, Harris suggested.
Virtual Medicare wellness exams for certain patients could also be valuable, especially for providers in ACOs. “When it's done at home, we're able to see some the home environments and other things they may be dealing with,” said Lilly.
It remains to be seen what telehealth flexibilities from CMS and private payers will last beyond the pandemic, but providers are advocating for greater telehealth support now that the technology is in more physician offices.
Other industry leaders are also using the crisis to promote wider transformation, like the end of fee-for-service reimbursement.
Physician practices, as well as large health systems, have had to furlough providers, eliminate positions, and reduce compensation for their staff due to the financial challenges from the recent outbreak. How healthcare is financed has been a major driver of these tough decisions.
“The bigger picture here is the overall fee-for-service world that we've lived in since the 1960s,” said Duncanson. “If we were paid more to take care of our population and get a fee based on our population of people, no one in healthcare would be having the crisis they're having now because the revenue would still be coming in. They'd be managing their population in a different way.”
In fact, practices faring better during the pandemic are ones with population-based payments.

“What we see in practices that are doing well right now is that the most beneficial relationship is one in which more than 50 percent of the income for primary care is based on a prospective, capitated payment that is risk-adjusted and not based on past fee-for-service performance,” Etz explained.
Practices with this type of reimbursement structure are under less financial strain than their fee-for-service peers partly because they have a “dependable revenue stream that allows them to do what primary care does best, which is to meet patients when and where they need through whatever modality,” Etz added.
Few providers earn population-based payments like the one Etz described. According to the latest report from the Health Care Payment Learning & Action Network, only 5.1 percent of healthcare payments made in 2019 came from a population-based payment method, including condition-specific population-based payments and comprehensive population-based payments.
The healthcare system has been earnestly moving away from fee-for-service for over a decade now, but the transition has been slow. Some providers hope the COVID-19 pandemic spurs private payers to reconsider their reimbursement methods to ensure steady, predictable payments for providers, especially those in primary care.
But regardless of how physician practices get paid, it is imperative to keep office doors open as physicians are finding themselves at greatest risk right before a major surge in demand for their services, Harris stated.
“Healthcare is a $3 trillion a year industry and just because of COVID doesn't mean that everything else is going to stop,” he said. “If independent practices and physicians across the board go out of business, who is going to be there to take care of all these patients and all their medical needs?”
“It's imperative that we get financial lifelines, so we can continue to keep our offices open, especially as we ramp up in the ensuing months as this COVID epidemic starts to taper down and the rest of medicine starts to pick up.”
For more coronavirus updates, visit our resource page, updated twice daily by Xtelligent Healthcare Media.
Dig Deeper on Medical billing and collections
-
![]()
Physicians' telehealth use varies across specialties, practice type
By: Anuja Vaidya
-
![]()
Which physicians are most likely to provide telehealth?
By: Anuja Vaidya
-
![]()
Primary, Specialty Care Physicians Favor Telehealth More Than Surgeons
By: Anuja Vaidya
-
![]()
Healthcare Providers, Patients Trust, Plan to Continue Telehealth Use



