clinical documentation

What is clinical documentation?
Clinical documentation (CD) is the creation of a digital or analog record detailing a medical treatment, medical trial or clinical test.
Clinical documents must be accurate, timely, and reflect specific services provided to a patient. Paper or digital documentation is often accompanied by supporting electronic files as electronically stored information, such as magnetic resonance imaging scans and X-rays (medical imaging), electrocardiograms (EKGs), and monitoring records.
Accuracy in clinical documentation is crucial for delivering high-quality patient care, supporting clinical decision-making using tools such as clinical decision support systems, and ensuring legal and regulatory compliance with laws such as the Health Insurance Portability and Accountability Act (HIPPA).
Facilitating inter-provider communication
Clinical documentation is used to facilitate inter-provider communication, allow evidence-based healthcare systems to automate decisions, provide evidence for legal records, and create patient registry functions so public health agencies can manage and research large patient populations more efficiently.
Clinical documentation is also used in the creation of longitudinal patient records (LEPRs), a type of electronic health record (EHR) that includes all healthcare information from all sources for an individual patient. By integrating comprehensive patient data, LEPRs help in tracking patient outcomes and improving the continuity of care.
Billing and coding applications
Billing and coding staff for healthcare providers use clinical documentation when evaluating claims. To ensure there are no gaps in a patient's clinical documentation, some healthcare facilities employ clinical document improvement (CDI) specialists to review each patient's clinical documentation and make certain it is comprehensive.
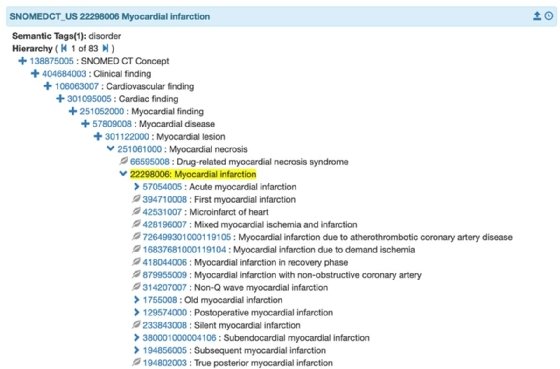
In the United States, billing departments are increasingly turning to clinical documentation improvement systems (CDIS) to improve the accuracy of clinical documentation and help ease the transition to the ICD-10 diagnosis coding language -- sometimes used in conjunction with Systematized Nomenclature of Medicine -- Clinical Terms (SNOMED CT). These systems enhance the precision of medical coding and ensure that healthcare providers receive appropriate reimbursement for their services.
The benefits of proper clinical documentation protocols
Maintaining proper clinical documentation procedures enhances the quality and completeness of clinical documentation. The benefits include the following:
- Improved patient care: Ensures accurate and comprehensive documentation, leading to better patient outcomes and care continuity.
- Better clinical outcomes: Facilitates precise diagnosis and treatment plans, contributing to improved clinical results.
- Enhanced compliance with regulatory requirements: Helps healthcare organizations meet standards and guidelines set by regulatory bodies, reducing the risk of compliance issues.
- Identification of documentation gaps: CD specialists work with healthcare providers to identify and rectify documentation deficiencies.
- Education on best practices: Provides ongoing training and education to healthcare providers on effective documentation practices.
Challenges and future trends in clinical documentation
Despite its benefits, clinical documentation faces several challenges, including the burden on healthcare providers and the need for continuous training and updates.
Future trends in clinical documentation include the integration of artificial intelligence (AI) and machine learning (ML) to streamline documentation processes and improve accuracy. These technologies have the potential to reduce administrative workload and enhance the overall quality of clinical documentation.
Generative AI in healthcare promises to ease tasks such as clinical documentation. Learn about three use cases for generative AI in healthcare documentation.






